Coronectomy Case Study – Third Molar Case and Biopsy
This case done by Dr. Wes Parker illustrates why it’s a good idea to have your third molars (wisdom teeth) evaluated by an Oral and Maxillofacial Surgeon and possibly removed. This was a 61 year old female who presented with pain and pericoronitis (a soft tissue infection commonly associated with wisdom teeth). She had an impacted tooth #32 (lower right third molar/wisdom tooth). She had 8 mm (deep) periodontal/gum pockets with bleeding on probing on the distal aspect of tooth #31. Her dentist as a teenager told her that she should not have her wisdom teeth removed. For the past 30 years, she reported periodic swelling and discomfort from the #32 area. She was referred to Dr. Parker by her new general dentist in 2019.

The Panoramic Radiograph Results:
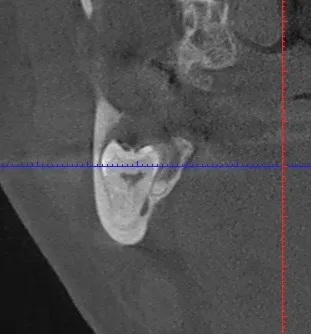
Her preoperative, panoramic radiograph showed a deeply impacted, distoangular tooth #32 with a well-defined, radiolucent (dark) lesion associated with the crown. The root apices of the tooth were in close proximity to the right inferior alveolar nerve and the inferior border of the mandible (lower jaw). We discussed doing an excisional biopsy of the lesion and a coronectomy of the tooth instead of an extraction in this case to both treat/remove the lesion and minimize the risk of nerve damage and a fracture of her mandible. A coronectomy procedure involves removing the crown and pulp contents of a noninfected, usually deeply impacted, wisdom tooth in order to minimize risk to the jaw and the nerve that provides sensation to the lower lip and chin. The roots are left in place during this procedure. This is in contrast to a standard extraction in which the entire tooth, crown and roots, are removed. Image #1 shows the patient’s preoperati
ve panoramic radiograph. Image #2 shows a coronal slice from her preoperative CBCT. Note the volume that the third molar occupies within her mandible, her thin bony cortices, and the proximity of the roots to both the right inferior alveolar nerve (lingual to roots) and the mandibular inferior border. Image #3 shows a one week po
The Biopsy Reveal:
At this time, the biopsy was revealed to be an infected dentigerous cyst. Dentigerous cysts are common, benign cysts that form around impacted teeth, most often third molars/wisdom teeth. If not removed, they can become quite large and destroy bone, and/or become secondarily infected. Image #4 shows a three month postoperative PA. Image #5 shows a six month postoperative PA. Note the radiographic bone fill in the area of the previous crown and lesion. The radiographs show some initial slight coronal (upward) migration of the root complex, which subsequently ceased. She is currently pain free, infection free, and has no periodontal probing depths greater than 2 mm on the distal of tooth #31. She is very happy and was gracious enough to allow us to share her case.